 the nursing station ایستگاه پرستاری
the nursing station ایستگاه پرستاری

Hypernatremia
هایپرناترمی در واقع به مقادیر بالاتر از حد طبیعی سدیم اطلاق می گردد. ( بیش از ۱۴۵ میلی اکی والان/ لیتر) . علت بروز آن ، دریافت سدیم بیشتر از آب و یا از دست رفتن آب بیشتر از سدیم می باشد . این عارضه ممکن است در بیمارانی با حجم طبیعی مایع یا در افراد دارای FVD یا FVE به وجود آید .
در موارد از دست دادن آب ، آب بیشتر از سدیم از بدن خارج می گردد ، در نتیجه غلظت سدیم سرم افزایش یافته و همین غلظت بالا موجب خارج شدن مایع از سلول می شود . این امر سبب بروز FVD داخل سلولی و خارج سلولی خواهد شد. در فزونی سدیم ، سدیم بیشتر از آب حفظ شده یا توسط بیمار به مصرف می رسد.
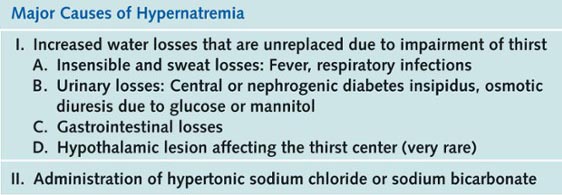
یکی از علل شایع هایپرناترمی ، محرومیت از مایع در بیماران بیهوش است که قادر به درک تشنگی نبوده ، نسبت به آن پاسخ نمی دهند و نمی توانند وجود آن را اظهار دارند. بیشتر افرادی که به این عارضه دچار می شوند خیلی جوان ، یا خیلی پیرند و یا بیمارانی هستند که دچار اختلالات شناختی شده اند.
تجویز مواد هایپرتونیک از راه لوله ، بدون مصرف مکمل های آب در حد کافی ، منجر به بروز هایپرناترمی می گردد ، همانگونه که اسهال های آبکی و افزایش شدید دفع نامحسوس آب (هایپرونتیلاسیون و اثرات برهنگی ناشی از سوختگی) می توانند این عارضه را بوجود آورند.
دیابت بی مزه ، عارضه ای با کمبود ADH در بخش خلفی غده هیپوفیز ایجاد می گردد ، در صورتیکه بیمار قادر به درک یا پاسخ نسبت به تشنگی نباشد و یا در موارد محدودیت شدید مصرف مایعات ، می تواند هایپرناترمی را ایجاد کند. در هنگام بررسی بیمار، علل نوروژنیک یا نفروژنیک دیابت بی مزه نیز باید مورد ملاحظه قرار گیرند.
- گرمازدگی
- قرار گرفتن در معرض خطر غرق شدن در آب دریا (غلظت سدیم در آب دریا تقریبا ۵۰۰ میلی اکی والان/ لیتر است)
- اختلال سیستم های تنظیم کننده ی نسبت در همودیالیزها یا دیالیزهای صفاقی
تجویز داخل وریدی سالین هایپرتونیک یا استفاده بیش از حد از بی کربنات سدیم نیز می تواند منجر به هایپرناترمی می گردد.
تظاهرات بالینی
- تظاهرات بالینی هایپرناترمی ، عمدتا عصبی بوده و به دنبال افزایش اسمولالیته پلاسما در اثر بالا رفتن سطح سدیم سرم پدید می آیند.
- هایپرناترمی نسبتا غلظت ECF را افزایش داده و سبب کشیده شدن آب به طرف خارج سلول می گردد.
- از نظر بالینی این تغییرات می توانند به صورت بی قراری و ضعف در هایپرناترمی های متوسط و عدم تشخیص موقعیت ، تصورات باطل و توهم در هایپرناترمی های شدید ، نمود پیدا کنند.
- کم آبی یا دهیدراتاسیون ( کم آبی که منجر به هایپرناترمی می گردد ) ، در افراد سالخورده ، اغلب به عنوان علت اولیه تغییرات رفتاری در نظر گرفته نشده و نسبت به آن بی توجهی می شود.
- اگر هایپرناترمی شدید باشد ، منجر به بروز صدمات مغزی دائمی و پایدار خواهد شد (خصوصا در کودکان) . صدمات مغزی ظاهرا ناشی از خونریزی های ناحیه زیر عنکبوتیه در اثر انقباضات مغزی می باشند.
 اولین مشخصه هایپرناترمی ، تشنگی است. تشنگی عاملی است که از سطح سدیم سرم به شدت محافظت می نماید و در نتیجه افراد سالم هرگز به هایپرناترمی دچار نمی شوند مگر آنکه فرد هوشیاری خود را از دست داده باشد یا از دسترسی به آب محروم باشد . متاسفانه در افراد بیمار، مکانیسم های تشنگی ممکن است دچار اختلال گردد.
اولین مشخصه هایپرناترمی ، تشنگی است. تشنگی عاملی است که از سطح سدیم سرم به شدت محافظت می نماید و در نتیجه افراد سالم هرگز به هایپرناترمی دچار نمی شوند مگر آنکه فرد هوشیاری خود را از دست داده باشد یا از دسترسی به آب محروم باشد . متاسفانه در افراد بیمار، مکانیسم های تشنگی ممکن است دچار اختلال گردد.
سایر علائم عبارتند از :
- خشکی و تورم زبان و چسبنده شدن غشاهای مخاطی
- پوست برافروخته
- ادم ریوی و محیطی
- هایپوتانسیون وضعیتی
- افزایش تونوس عضلانی و رفلکس های تاندون عمقی
- درجه حرارت بدن هم ممکن است در حد ضعیف افزایش یابد که با اصلاح هایپرناترمی ، به وضعیت طبیعی باز می گردد.
در هایپرناترمی ، سطح سدیم سرم بالغ بر ۱۴۵ میلی اکی والان / لیتر و اسمولالیته سرم نیز بیش از ۳۰۰ میلی اسمول/ کیلوگرم می باشد. با تلاش کلیه جهت حفظ آب ( به شرط آنکه از دست رفتن آب در مکانی به جز کلیه صورت گیرد) وزن مخصوص ادرار و اسمولالیته ادرار نیز افزایش می یابد.
درمان هایپرناترمی عبارتست از :
پائین آوردن تدریجی سطح سدیم ادرار از طریق تزریق محلول الکترولیتی هایپوتونیک (مثلا کلراید سدیم ۰٫۴۵ %) یا محلول ایزوتونیک بدون نمک (مثل دکستروز ۵% در آب). D5W زمانی مورد استفاده قرار می گیرد که فقط به جایگزینی آب بدون سدیم نیاز باشد .
از نظر بسیاری از پزشکان ، محلول سدیم هایپوتونیک خطر کمتری نسبت به D5W دارد چون سبب کاهش تدریجی سطح سدیم سرم شده و در نتیجه خطر ادم مغزی را کاهش می دهد.
این محلول ، محلول انتخابی در موارد بروز هایپرگلیسمی های شدید همراه با هایپرناترمی می باشد. کاهش سریع سطح سدیم سرم ، سبب کاهش موقت اسمولالیته پلاسما می گردد به نحوی که میزان آن به پائین تر از حدی می رسد که در مایع درون بافتهای مغز وجود دارد و همین امر ادم مغزی خطرناکی را ایجاد می نماید. همچنین برای درمان مقادیر سدیم دریافت شده، داروهای مدر را تجویز می کنند.
در رابطه با اینکه سطح سدیم سرم تا چه حد باید کاهش پیدا کند ، هنوز میزان دقیقی ارائه نشده است. بر مبنای یک قانون عمومی ، سرعت کاهش سدیم سرم نباید بیشتر از ۰٫۵ تا ۱ میلی اکی والان / لیتر باشد تا زمان کافی برای تنظیم و تعدیل مجدد بخش های مختلف مایع از طریق انتشار، فراهم آید.
- اگر علت هایپرناترمی ، دیابت بی مزه باشد ، دسموپرسین (DDAVP) تجویز می شود . (دسموپرسین یک هومرمون ضد ادراری صناعی است).
- راه های جذب و دفع مایع در بیماران در معرض خطر بروز هایپرناترمی باید تحت کنترل و مراقبت دقیق قرار گیرند.
- پرستار باید موارد دفع غیر طبیعی آب یا مصرف مقادیر کم آب و دریافت زیاد سدیم را که ممکن است در اثر استفاده از داروهای بدون نسخه حاوی سدیم زیاد بوجود آمده باشد مورد بررسی قرار دهد.
- علاوه بر آن گرفتن تاریخچه ای داروهای مصرفی نیز حائز اهمیت می باشد چون برخی داروهای تجویز شده ممکن است حاوی مقادیر زیادی سدیم باشند.
- علاوه بر این ها، پرستار وجود تشنگی یا بالا رفتن دمای بدن را در بیمار ثبت نموده و ارتباط آنها را با سایر علائم بالینی، ارزیابی می نماید.
- همچنین تغییرات رفتاری، نظیر بی قراری ، عدم تشخیص موقعیت و خواب آلودگی نیز باید توسط پرستار، نظارت دقیق صورت گیرد.
- پرستار جهت پیشگیری از هایپرناترمی ، باید تلاش نماید تا طی فواصل زمانی منظم ، مایعات در اختیار بیمار قرار دهد ، خصوصا در بیماران دچار ضعف و ناتوانی که قادر به درک تشنگی یا نشان دادن واکنش نسبت به آن نیستند .
- اگر مصرف مایعات همچنان ناکافی بود ، پرستار باید برای انتخاب روش دیگر جهت مصرف مایع ، یعنی تغذیه با لوله یا تزریق داخل وریدی مایع ، با پزشک مشورت نماید.
- اگر تغذیه بیمار از راه لوله صورت می گیرد ، باید مقادیر کافی آب نیز تجویز شود تا میزان BUN و سدیم سرم در حد طبیعی باقی بماند .
- به عنوان یک قانون کلی ، هر چه اسمولالیته مواد غذایی داده شده از راه لوله بیشتر باشد ، نیاز به مکمل های آب نیز افزایش خواهد یافت.
- در بیماران مبتلا به دیابت بی مزه ، باید از مصرف آب به میزان کافی اطمینان حاصل کرد.
- اگر بیمار هوشیار بوده و مکانیسم های تشنگی در وی دچار آسیب نشده است ، در آن صورت فقط دسترسی وی به آب میتواند کافی باشد.
- در صورت کاهش سطح هوشیاری بیمار یا بروز سایر ناتوانایی هایی که می تواند بر مصرف کافی مایعات ، تاثیر گذارد ، مایعات تزریقی جایگزین می شود.
- این نوع درمان را برای بیماران مبتلا به اختلالات عصبی ، به ویژه در مراحل اولیه پس از عمل جراحی ، میتوان تدارک دید.
وقتی برای کنترل هایپرناترمی استفاده از مایعات تزریقی ضرورت پیدا می کند ، در آن صورت پرستار باید از طریق مطالعه مقادیر سریال سرم و با مشاهده تغییرات بوجود آمده در علائم عصبی ، پاسخ بیمار را نسبت به مایعات کنترل نماید.
با کاهش تدریجی میزان سدیم سرم ، علائم عصبی باید بهبود یابند. همانگونه که در مباحث پیشین شرح داده شد ، کاهش سریع میزان سدیم سرم، سبب هایپواسموتیک شدن موقت پلاسما در مقایسه با مایعات بافتی مغز می گردد ، که میتواند ادم مغزی خطرناکی را بوجود آورد.
 Hypernatremia
Hypernatremia
Hypernatremia, a less common problem than hyponatremia, refers to an excess of sodium relative to the amount of water in the body. Severe hypernatremia can lead to seizures, coma, and permanent neurologic damage
How it happens
Thirst is the body’s main defense against hypernatremia. The hypothalamus (with its osmoreceptors) is the brain’s thirst center. High serum osmolality (increased solute concentrations in the blood ) stimulates the hypothalamus and initiates the sensation of thirst.
The drive to respond to thirst is so strong that severe, persistent hypernatremia usually occurs only in people who can’t drink voluntarily, such as infants, confused elderly patients, and immobile or unconscious patients. Hypothalamic disorders, such as a lesion on the hypothalamus, may cause a disturbance of the thirst mechanism, but this condition is rare. When hypernatremia occurs, it usually has a high mortality rate (greater than 50%).
Striving for balance
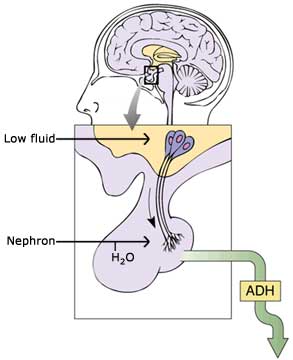
The body strives to maintain a normal sodium level by secreting ADH from the posterior pituitary gland. This hormone causes water to be retained, which helps to lower serum sodium levels.
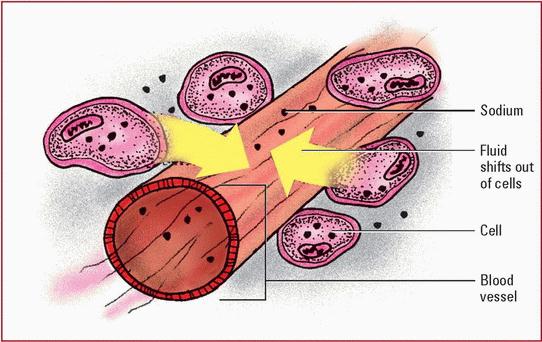
The cells also play a role in maintaining sodium balance. When serum osmolality increases because of hypernatremia, fluid moves by osmosis from inside the cell to outside the cell, to balance the concentrations in the two compartments.
As fluid leaves the cells, they become dehydrated and shrink especially those of the CNS. When this occurs, patients may show signs of neurologic impairment. They may also show signs of hypervolemia (fluid overload) from increased extracellular fluid volume in the blood vessels. If the overload is severe enough, subarachnoid hemorrhage may occur.
Increased concentration
A water deficit can cause hypernatremia that is, more sodium relative to water in the body. Excessive intake of sodium can also cause it. Regardless of the cause, body fluids become hypertonic (more concentrated).
Water deficit
A water deficit can occur alone or with a sodium loss (but more water is lost than sodium). In either case, serum sodium levels are elevated. This elevation is more dangerous in debilitated patients and those with deficient water intake.
Insensible water losses of several liters per day can result from fever and heat stroke, with older adults and athletes being equally susceptible. Significant water losses also occur in patients with pulmonary infections, who lose water vapor from the lungs through hyperventilation, and in patients with extensive burns. Vomiting and severe, watery diarrhea are other causes of water loss and subsequent hypernatremia; either can be especially dangerous in children.
Ages and stages
Infants, children, and elderly patients at risk
Hypernatremia is more common in infants and children for two key reasons:
۱ ) They tend to lose more water as a result of diarrhea, vomiting, inadequate fluid intake, and fever.
۲ ) Their intake of water is generally inadequate because they have difficulty swallowing, lack access to fluids, and can’t readily communicate their needs.
Elderly patients are also at increased risk for hypernatremia. They may have an impaired thirst response, or they may have limited access to water because of confusion, immobility, or a debilitating illness.
- Patients with hyperosmolar hyperglycemic nonketotic syndrome (HHNS) can also develop hypernatremia due to severe water losses from osmotic diuresis.
- Urea diuresis, another cause of hypernatremia, occurs with administration of high-protein feedings or high-protein diets without adequate water supplementation.
Thirst to an extreme
Patients with diabetes insipidus have extreme thirst and enormous urinary losses, in many cases more than 4 gal (15 L)/day. Usually, they can drink enough fluids to match the urinary losses; otherwise, severe dehydration and hypernatremia occur. Diabetes insipidus may result from a lack of ADH from the brain (central diabetes insipidus) or a lack of response from the kidneys to ADH (nephrogenic diabetes insipidus).
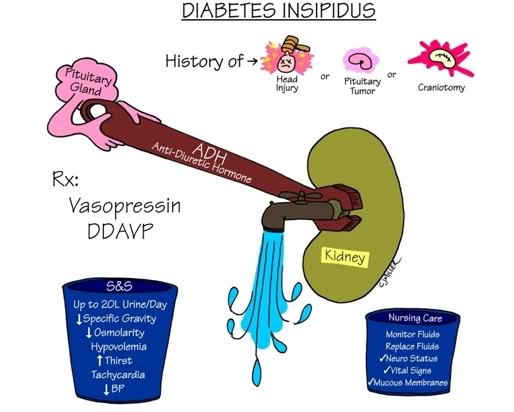
- Central diabetes insipidus may be caused by a tumor or head trauma (injury or surgery), or it may be idiopathic (no known cause). It responds well to vasopressin (another name for ADH).
- nephrogenic diabetes insipidus doesn’t respond well to vasopressin and is more likely to occur with an electrolyte imbalance such as hypokalemia or with certain medications such as lithium.
Drugs associated with hypernatremia
The drugs listed below can cause high sodium levels. Ask your patient if any of these medications are part of his drug therapy:
- antacids with sodium bicarbonate
- antibiotics such as ticarcillin disodiumclavulanate potassium (Timentin)
- salt tablets
- sodium bicarbonate injections (such as those given during cardiac arrest)
- I.V. sodium chloride preparations
- sodium polystyrene sulfonate (Kayexalate).
Excessive sodium intake
Like water losses from the body, sodium gains can cause hypernatremia. Several factors can contribute to a high sodium level, including salt tablets, high-sodium foods, and medications such as sodium polystyrene sulfonate (Kayexalate). Excessive parenteral administration of sodium solutions, such as hypertonic saline solutions or sodium bicarbonate preparations, and gastric or enteral tube feedings can also cause hypernatremia.

Other causes of increased sodium levels include inadvertent introduction of hypertonic saline solution into maternal circulation during therapeutic abortion and near drowning in salt water. Excessive amounts of adrenocortical hormones (as in Cushing’s syndrome and hyperaldosteronism) also affect water and sodium balance.
What to look for
The most important signs of hypernatremia are neurologic because fluid shifts have a significant effect on brain cells. Remember, the body can tolerate a high sodium level that develops over time better than one that occurs rapidly.
Early signs and symptoms of hypernatremia may include :
- restlessness or agitation
- anorexia
- nausea
- vomiting
These may be followed by :
- weakness
- lethargy
- confusion
- stupor
- seizures
- coma
Neuromuscular signs also commonly occur, including :
- twitching
- hyperreflexia
- ataxia
- tremors
That flushed, fevered feeling
You may also observe a low-grade fever and flushed skin. The patient may complain of intense thirst from stimulation of the hypothalamus from increased osmolality.
Other signs and symptoms vary depending on the cause of the high sodium levels. If a sodium gain has occurred, fluid may be drawn into the blood vessels and the patient will appear hypervolemic, with an elevated blood pressure, bounding pulse, and dyspnea.
If water loss occurs, fluid leaves the blood vessels and you’ll notice signs of hypovolemia, such as :
- dry mucous membranes
- oliguria
- orthostatic hypotension (blood pressure drop and heart rate increase with position changes).
Memory jogger
To remember some common signs and symptoms of hypernatremia, think of the word SALT:
- Skin flushed
- Agitation
- Low-grade fever
- Thirst.
What tests show
Now that you know how hypernatremia progresses, you can better understand how it causes these common diagnostic findings:
- serum sodium level greater than 145 mEq/L
- urine specific gravity greater than 1.030 (except in diabetes insipidus, where urine specific gravity is decreased)
- serum osmolality greater than 300 mOsm/kg
How it’s treated
Treatment Treatment for hypernatremia varies with the cause. The underlying disorder must be corrected, and serum sodium levels and related diagnostic tests must be monitored. If too little water in the body is causing the hypernatremia, treatment may include oral fluid replacement.

- Note that the fluids should be given gradually over 48 hours to avoid shifting water into brain cells.
- Remember, as sodium levels in the blood vessels rise, fluid shifts out of the cells including the brain cells to dilute the blood and equalize concentrations.
- If too much water is introduced into the body too quickly, water moves into brain cells and they get bigger, causing cerebral edema .
- If the patient can’t drink enough fluids, he’ll need I.V. fluid replacement.
- He may receive salt-free solutions (such as dextrose 5% in water) to return serum sodium levels to normal, followed by infusion of half-normal saline solution to prevent hyponatremia and cerebral edema.
- Other treatments include restricting sodium intake and administering diuretics along with oral or I.V. fluid replacement to increase sodium loss.
- Treatment for diabetes insipidus may include vasopressin, hypotonic I.V. fluids, and thiazide diuretics to decrease free water loss from the kidneys. The underlying cause should also be treated.
How you intervene
Try to prevent hypernatremia in high-risk patients (such as those recovering from surgery near the pituitary gland) by observing them closely. Also find out if they’re taking medications that may cause hypernatremia. If your patient does develop hypernatremia, take the following measures:
• Monitor and record vital signs, especially blood pressure and pulse.
• If the patient needs I.V. fluid replacement, monitor fluid delivery and his response to the therapy. Watch for signs of cerebral edema and check his neurologic status frequently. Report any deterioration in LOC.
• Carefully measure and record intake and output. Weigh the patient daily to check for body fluid loss.
• Assess skin and mucous membranes for signs of breakdown and infection as well as water loss from perspiration.
• Monitor the patient’s serum sodium level and report any increase. Monitor urine specific gravity and other laboratory test results.
• If the patient can’t take oral fluids, recommend the I.V. route to the practitioner. If the patient can drink and is alert and responsible, involve him in his treatment. Give him a target amount of fluid to drink each shift, mark cups with the volume they hold, leave fluids within easy reach, and provide paper and pen to record amounts. If family members want to help the patient drink, give them specific instructions as well.
• Insert and maintain a patent I.V. as ordered. Use an infusion pump to control delivery of I.V. fluids to prevent cerebral edema.
• Assist with oral hygiene. Lubricate the patient’s lips frequently with a water-based lubricant and provide mouthwash or gargle if he’s alert. Good mouth care helps keep mucous membranes moist and decreases mouth odor.
• Provide a safe environment for confused or agitated patients. If seizures are likely, pad the bed’s side rails and keep an artificial airway and suction equipment handy. Reorient the patient as needed, and reduce environmental stimuli.
- Chart smart
- Teaching points
Documenting hypernatremia
If your patient has hypernatremia, make sure you document the following information:
- assessment findings (including neurologic status)
- vital signs
- types of seizures, if any
- daily weight
- serum sodium level and other pertinent laboratory test results
- intake and output
- medications given and I.V. therapy implemented
- notification of the practitioner when the patient’s condition changes
- nursing interventions and patient response
- patient compliance with fluid restrictions and dietary changes
- patient teaching provided and patient response to the teaching
- safety measures taken to protect the patient (seizure precautions).
Teaching about hypernatremia
When teaching a patient with hypernatremia, be sure to cover the following topics and then evaluate your patient’s learning:
- explanation of hypernatremia, including causes and treatment
- importance of restricting sodium intake, including both dietary sources and over-thecounter medications that contain sodium
- drug therapy and possible adverse effects
- signs and symptoms and when to report them.
منبع : برونر و سودارث ( ویرایش یازدهم ۲۰۰۸ ) درد ، الکترولیت ، شوک ، سرطان ، مراقبت پایان عمر
مترجمان : دکتر ژیلا عابد سعیدی و نیره ابراهیمی ، دکتر زهره پارسا یکتا ، منصوره فراهانی ، زهرا تذکری
Fluids & Electrolytes made Incredibly Easy ! ®, ۵th Edition
Copyright ©۲۰۱۱ Lippincott Williams & Wilkins
تهیه و تنظیم : مرضیه براهویی و صادق دهقانی زاده






عالی بود دمتون گرم