 the nursing station ایستگاه پرستاری
the nursing station ایستگاه پرستاری
Hyperphosphatemia
هایپرفسفاتمی به مقادیر بالاتر از حد طبیعی فسفر سرم اطلاق می شود. وضعیتهای گوناگونی منجر به بروز این عدم توازن می گردد ، اما شایع ترین آن نارسایی کلیوی است . علل دیگر شامل :- افزایش جذب و کاهش دفع
- انتقال از فضای داخل سلولی به فضای خارج سلولی
- شیمی درمانی بیماران نئوپلاستیک
- کاهش ترشح هورمون پاراتیروئید
- اسیدوز تنفسی یا کتواسیدوزدیابتیک
- همولیز حاد
- مصرف مقادیر زیاد فسفات
- نکروز شدید عضلانی و افزایش جذب فسفر
- بالا رفتن میزان فسفر سرم نشانه های اندکی ایجاد می نماید .
- نشانه های بوجود آمده نیز معمولا ناشی از کاهش کلسیم و کلسیفیکاسیون بافت نرم است.
- مهمترین پیامد این اختلال تتانی است که از جمله عوارض زودرس به شمار می آید .
- به دلیل ارتباط دو جانبه ای که میان فسفر و کلسیم وجود دارد ، مقادیر بالای فسفر سرم ، موجب کاهش غلظت کلسیم سرم می گردد.
- تتانی موجب بروز احساس سوزن سوزن شدن در نوک انگشتان دست و اطراف دهان می شود .
- بی اشتهایی ، تهوع ، استفراغ ، ضعف عضلانی ، درد عضلات و مفاصل ، افزایش فعالیت های رفلکسی و افزایش ضربان های قلب نیز ممکن است به وقوع بپیوندد.
از عوارض دیررس می توان به کلسیفیکاسیون بافت نرم اشاره کرد که عمدتا در بیمارانی که میزان تصفیه گلومرولی در آنها کاهش یافته ، ایجاد می شود. مقادیر بالای فسفر غیر ارگانیک در سرم ، سبب رسوب فسفات کلسیم در مناطق غیر استخوانی شده و برون ده ادراری را کاهش می دهد . علاوه بر این موجب بروز اختلالات بینایی و تپش قلب می گردد.
- در آنالیز آزمایشگاهی ، مقادیر فسفر سرم بزرگسالان بیش از ۴٫۵ میلی گرم / دسی لیتر گزارش می شود.
- مقادیر فسفر سرم به طور طبیعی در کودکان ، بالاتر است که این امر ناشی از سرعت بالای رشد استخوانی است .
- اندازه گیری مقادیر کلسیم سرم نیز برای تشخیص مشکل اولیه و بررسی اثرات ناشی از درمان می تواند مفید باشد .
- بررسی های رادیولوژی با کمک اشعه X نشان دهنده تغییرات اسکلتی همراه با رشد غیر طبیعی استخوان است.
- در هایپوپاراتیروئیدیسم مقادیر PTH کاهش می یابد .
- برای ارزیابی عملکرد کلیه ، BUN و کراتنین را هم اندازه گیری می کنند.
- انجام سونوگرافی از کلیه ها به عنوان بخشی از بررسی های تشخیصی نارسایی کلیوی ، کلسیفیکاسیون شریان های کرونر هم اطلاعاتی در مورد ویژگی مزمن بودن نارسایی کلیه و پیش آگهی آن در اختیار قرار می دهد.
در صورت امکان ، درمان با هدف علاج اختلالات زمینه ساز و اصلی صورت می گیرد . به عنوان مثال ، هایپرفسفاتمی ممکن است در ارتباط با کاهش حجم یا اسیدوز متابولیک یا تنفسی ایجاد گردد. در نارسایی کلیوی ، افزایش تولید هورمون پاراتیروئیدی در افزایش میزان فسفر و بیماری استخوانی دخالت دارد.
- اقدامات مربوط به پائین آوردن مقادیر فسفات سرم در این بیماران شامل استفاده از فرآورده های ویتامین D نظیر کلسیتریول (که به صورت خوراکی [روکالترول] و تزریقی [کالسی جکس، پاری کالسیتول[زمپلاز] ]موجود می باشد) است.
- کلسیتریول IV سبب افزایش کلسیم سرم نمی گردد ، بلکه شرایط را برای انجام درمان های تهاجمی تر هایپرفسفاتمی نظیر مصرف آنتی اسید های باند شده با کلسیم (کلسیم کربنات یا کلسیم سیترات) ، ژلها یا آنتی اسیدهای باند شده با فسفات ، محدودیت مصرف مواد غذایی حاوی فسفات ، دیالیز، دیورز ایجاد شده توسط داروهای مدر حلقوی و کاهش حجم با کمک سالین فراهم می آورد . برای خارج کردن رسوبات وسیع کلسیم فسفری جراحی ضرورت پیدا می کند.
- پرستار باید بیماران در معرض خطر هایپرفسفاتمی را تحت مراقبت دقیق قرار دهد.
- وقتی رژیم غذایی کم فسفر برای بیمار تجویز می شود ، باید به وی آموزش داد تا از مصرف غذاهای سرشار از فسفر نظیر پنیر سفت ، خامه ، گوشت قرمز، آجیل ، غلات سبوس دار، میوه ها و سبزیجات خشک شده ، قلوه ، ساردین ، برخی ارگانهای حیوانی و غذاهای تهیه شده از شیر، خودداری نماید.
- در موارد مقتضی پرستار می تواند به بیمار در رابطه با پرهیز از موادی نظیر مسهل ها و تنقیه های محتوی فسفات ، آموزش دهد .
- به علاوه در رابطه با شناسایی علائمی که نشان دهنده قریب الوقوع بودن هایپوکلسمی است ، همچنین کنترل تغییرات بوجود آمده در برون ده ادرار، آموزش های لازم توسط پرستار به بیمار داده می شود.
Hyperphosphatemia
Hyperphosphatemia occurs when serum phosphorus levels exceed 4.5 mg/dl (or 2.6 mEq/L) and usually reflects the kidneys’ inability to excrete excess phosphorus. The condition commonly occurs along with an increased release of phosphorus from damaged cells. Severe hyperphosphatemia occurs when the serum phosphorus levels reach 6 mg/dl or higher.
Hyperphosphatemia can result from a number of underlying mechanisms, including impaired renal excretion of phosphorus, a shift of phosphorus from the intracellular fluid to the extracellular fluid, and an increase in dietary intake of phosphorus.
- Kidney filter failure
- PTH problem
- Shift work
- Increased intake
Normally, renal excretion of phosphorus equals the amount the GI tract absorbs daily. Hyperphosphatemia most commonly results from renal failure due to the kidneys’ inability to excrete excess phosphorus.
When glomerular filtration rate drops below 30 ml/minute, the kidneys can’t filter excess phosphorus adequately. Because the kidneys are responsible for most of the excretion of phosphorus, their inability to filter phosphorus leads to an elevated serum phosphorus level.
A risk after thyroid or parathyroid surgery, hypoparathyroidism impairs synthesis of PTH. When less PTH is synthesized, less phosphorus is excreted from the kidneys. The result?
- Elevated serum phosphorus levels.
Several conditions can cause phosphorus to shift from the intracellular fluid to the extracellular fluid. Acid-base imbalances, such as respiratory acidosis and DKA, are common examples. Anything that causes cellular destruction can also result in a transcellular shift of phosphorus. Destruction of cells can trigger the release of intracellular phosphorus into extracellular fluid, causing serum phosphorus levels to rise.
- Chemotherapy, for example, causes significant cell destruction, as do muscle necrosis and rhabdomyolysis, conditions that can stem from infection, heat stroke, and trauma.
Excessive intake of phosphorus can result from overadministration of phosphorus supplements or of laxatives or enemas that contain phosphorus (such as Fleet enemas).
- In infants, excessive intake of vitamin D can result in increased absorption of phosphorus and lead to elevated serum phosphorus levels.
Drugs associated with hyperphosphatemia
The following drugs may cause hyperphosphatemia:
- enemas such as Fleet enemas
- laxatives containing phosphorus or phosphate
- oral phosphorus supplements (Neutra-Phos)
- parenteral phosphorus supplements (sodium phosphate, potassium phosphate)
- vitamin D supplements.
Infants who are fed cow’s milk are predisposed to hyperphosphatemia because cow’s milk contains more phosphorus than breast milk. In addition, infants have naturally higher phosphorus levels.
Hyperphosphatemia causes few clinical problems by itself. However, phosphorus and calcium levels have an inverse relationship: If one is high, the other is low. Because of this seesaw relationship, hyperphosphatemia may lead to hypocalcemia, which can be life-threatening. Signs and symptoms of acute hyperphosphatemia are usually caused by the effects of hypocalcemia.
- The patient may develop paresthesia in the fingertips and around the mouth, which may increase in severity and spread proximally along the limbs and to the face.
- Severe muscle spasm, cramps, pain, and weakness may prevent the patient from performing normal activities.
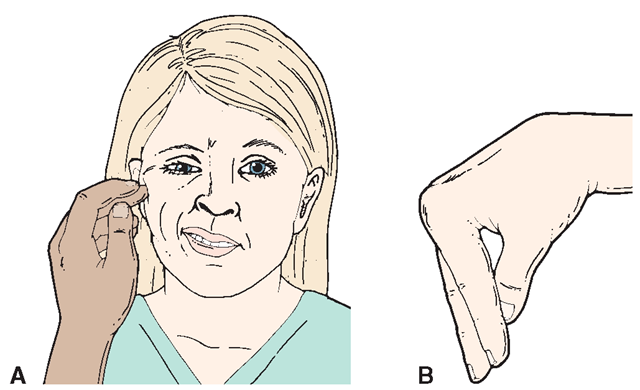
- The patient may exhibit hyperreflexia and positive Chvostek’s and Trousseau’s signs. These signs are due to low calcium levels and may progress to tetany and neurologic disorders.
- Cardiac irregularities
- Hyperreflexia
- Eating poorly
- Muscle weakness
- Oliguria.
Neurologic signs and symptoms include decreased mental status, delirium, and seizures. Electrocardiogram (ECG) changes include a prolonged QT interval and ST segment. The patient may also experience hypotension, heart failure, anorexia, nausea, and vomiting. Bone development may also be affected.
Calcification cues
When phosphorus levels rise, phosphorus binds with calcium, forming an insoluble compound called calcium phosphate. Organ dysfunction can result when calcium phosphate precipitates, or is deposited, in the heart, lungs, kidneys, or other soft tissues. This process, called calcification, usually occurs as a result of chronically elevated phosphorus levels.
With calcification, the patient may experience arrhythmias, an irregular heart rate, and decreased urine output. Corneal haziness, conjunctivitis, cataracts, and impaired vision may occur, and papular eruptions may develop on the skin.
What tests show
The following diagnostic tests results may indicate hyperphosphatemia or a related condition such as hypocalcemia :
- serum phosphorus level above 4.5 mg/dl (or 2.6 mEq/L)
- serum calcium level below 8.5 mg/dl
- X-ray studies that reveal skeletal changes due to osteodystrophy (defective bone development) in chronic hyperphosphatemia
- increased blood urea nitrogen (BUN) and creatinine levels, which reflect worsening renal function
- ECG changes characteristic of hypocalcemia (such as a prolonged QT interval).
How it’s treated
An elevated serum phosphorus level may be treated with drugs and other therapeutic measures. Treatment aims to correct the underlying disorder, if one exists, and correct hypocalcemia.
Going low phospho : If a patient’s elevated serum phosphorus level results from excessive phosphorus intake, the condition may be easily remedied by reducing phosphorus intake. Therapeutic measures include reducing dietary intake of phosphorus and eliminating the use of phosphorus-based laxatives and enemas. (See When dietary changes aren’t enough.)
Altering absorption : Drug therapy may help decrease absorption of phosphorus in the GI system. Such therapy may include aluminum, magnesium, or calcium gel or phosphate-binding antacids. Although widely used, such calcium salts as calcium carbonate and calcium acetate may cause hypercalcemia, so the patient will need careful dosing. Polymeric phosphate binders such as sevelamerhydrochloride may also be given. A patient with underlying renal insufficiency or renal failure should not receive magnesium antacids because they may cause hypermagnesemia. A patient with end-stage renal disease may receive lanthanum carbonate, a non-calcium, non-aluminum phosphate binder. Keep in mind that a mildly elevated phosphorus level may benefit a patient with renal failure . Higher phosphorus levels (on the higher side of the normal range) allow more oxygen to move from the RBCs to tissues, which can help prevent hypoxemia and limit the effects of chronic anemia on oxygen delivery.
Treat what’s underneath : Treatment of the underlying cause of hyperphosphatemia, including conditions such as respiratory acidosis or DKA, can lower serum phosphorus levels. In a patient with diabetes, administering insulin causes phosphorus to shift back into the cells, which can result in decreased serum phosphorus levels.
Situation:severe Patients with severe hyperphosphatemia may receive I.V. saline solution to promote renal excretion of phosphorus. However, this treatment requires the patient to have functional kidneys and the ability to tolerate the increased load of sodium and fluid. Patients may also receive proximal diuretics such as acetazolamide to increase renal excretion of phosphorus.
As a final therapeutic intervention, hemodialysis or peritoneal dialysis may be initiated if the patient has chronic renal failure or an extreme case of acute hyperphosphatemia with symptomatic hypocalcemia.
How you intervene
Keep an eye out for patients at risk for hyperphosphatemia, and monitor them carefully. Also, use care when administering phosphorus in I.V. infusions, enemas, and laxatives because the extra phosphorus may cause hyperphosphatemia.
If your patient has already developed hyperphosphatemia, your care should focus on careful monitoring, safety measures, and interventions to restore normal serum phosphorus levels. Follow these steps to provide care for the patient:
• Monitor vital signs.
• Watch for signs and symptoms of hypocalcemia, such as paresthesia in the fingers or around the mouth, hyperactive reflexes, or muscle cramps. If any of these occur, immediately notify the doctor. (See Teaching about hyperphosphatemia.) Also notify the practitioner if you detect signs or symptoms of calcification, including oliguria, visual impairment, conjunctivitis, irregular heart rate or palpitations, and papular eruptions.
• Monitor fluid intake and output. If urine output falls below 30 ml/hour, immediately notify the practitioner. Decreased urine output can seriously affect renal clearance of excess serum phosphorus.
• Closely monitor serum electrolyte levels, especially calcium and phosphorus. Report changes immediately. Also monitor BUN and serum creatinine levels because hyperphosphatemia can impair renal tubules when calcification occurs.
• Keep a flow sheet of daily laboratory test results for a patient at risk. Include BUN and serum phosphorus, calcium, and creatinine levels as well as fluid intake and output. Keep the flow sheet on a clipboard so changes can be detected immediately. (See Documenting hyperphosphatemia.)
• Administer prescribed medications, monitor their effectiveness, and assess the patient for possible adverse reactions. Give antacids with meals to increase their effectiveness in binding phosphorus.
• Prepare the patient with severe hyperphosphatemia for possible dialysis.
• If a patient’s condition results from chronic renal failure or if his treatment includes a low-phosphorus diet, consult a dietitian to help the patient comply with dietary restrictions. Dietary phosphorus should be restricted to 0.6 to 0.9 g/day.
- Teaching points
- Chart smart
When teaching a patient with hyperphosphatemia, be sure to cover the following topics and then evaluate your patient’s learning :
- causes and treatment
- prescribed medications
- avoidance of preparations that contain phosphorus, such as laxatives, enemas, and supplements
- avoidance of high-phosphorus foods, such as dairy products, organ meats, fish, poultry, eggs, and nuts and seeds
- warning signs and symptoms
- referrals to a dietitian and social services, if indicated.
If your patient has hyperphosphatemia, make sure you document the following information :
- all assessment findings
- intake and output
- I.V. therapy and medications given
- muscle spasms, cramps, pain, and muscle strength
- paresthesia in the fingertips and around the mouth
- visual disturbances
- safety measures to protect patient
- notification of the practitioner
- your interventions, including patient teaching and the patient’s response.
منبع : برونر و سودارث ( ویرایش یازدهم ۲۰۰۸ ) درد ، الکترولیت ، شوک ، سرطان ، مراقبت پایان عمر
مترجمان : دکتر ژیلا عابد سعیدی و نیره ابراهیمی ، دکتر زهره پارسا یکتا ، منصوره فراهانی ، زهرا تذکری
Fluids & Electrolytes made Incredibly Easy ! ®, ۵th Edition
Copyright ©۲۰۱۱ Lippincott Williams & Wilkins
تهیه و تنظیم : مرضیه براهویی و صادق دهقانی زاده